Case 1: Metastatic Disease
Clinical History
Patient: 72-year-old male History: Newly diagnosed Prostate Cancer (Gleason 4+4=8), PSA 45 ng/mL Indication: Staging for distant metastases
Imaging Findings
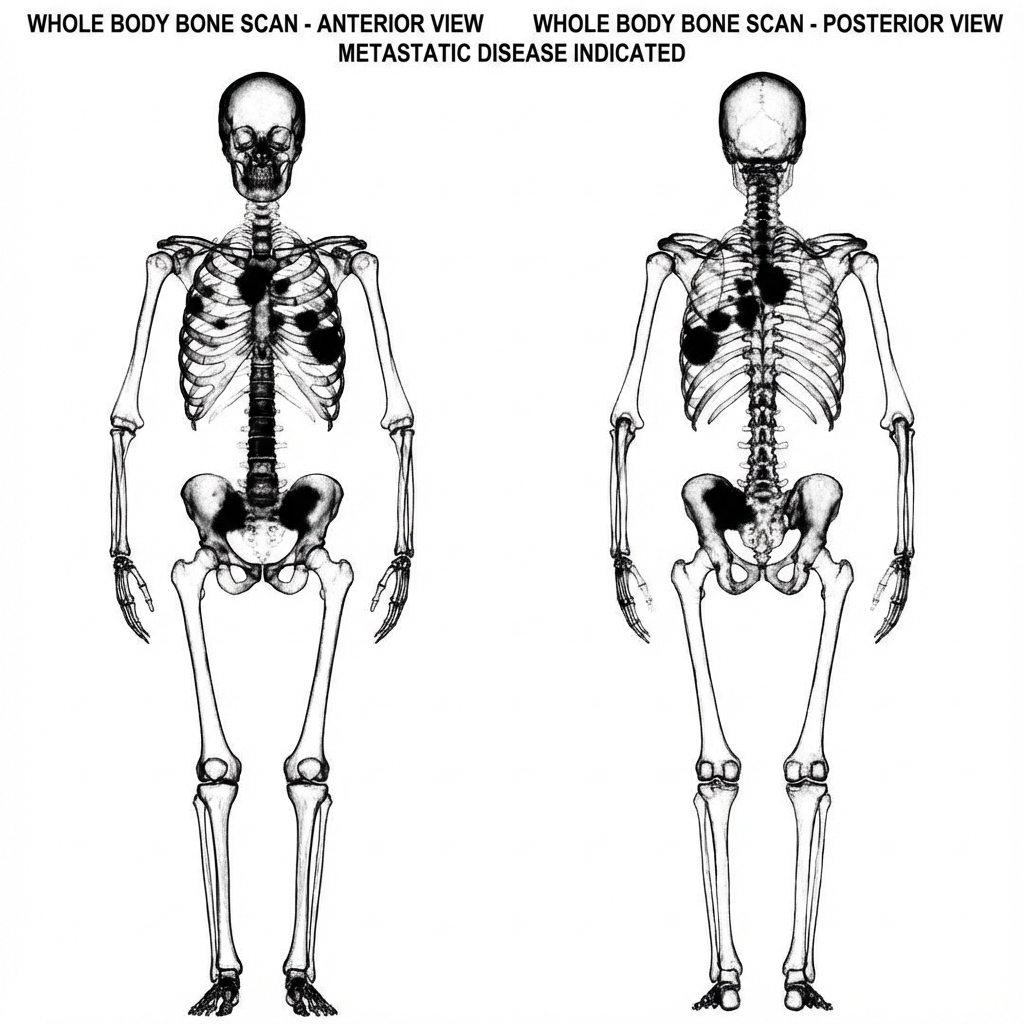
Technique: Whole Body Bone Scan (Tc-99m MDP)
Planar Images (Anterior & Posterior)
The scan reveals multiple, intense, focal areas of increased radiotracer uptake (“hot spots”) involving:
- Multiple bilateral ribs
- Thoracic and Lumbar spine (vertebral bodies)
- Right hemipelvis (ilium) and left ischium
- Proximal left femur
The kidneys are faintly visualized (normal excretion), but renal uptake is somewhat diminished relative to bone uptake (suggesting high skeletal burden).
Diagnosis
Findings:
- Random, multifocal distribution specifically affecting the axial skeleton.
- Typical “metastatic pattern”.
Interpretation: Diffusely metastatic bony disease.
Learning Points
- Distribution: Metastases typically affect the red marrow-containing axial skeleton (spine, pelvis, ribs, skull, proximal femurs/humeri).
- Pattern Recognition: Random, asymmetric, multifocal uptake is the classic appearance.
- Superscan vs. High Burden: A true “superscan” (diffuse involvement) might show absent kidneys. Here, high burden is key.
- Differential: Degenerative change correlates with joint spaces (knees, spine facets, shoulders). Trauma aligns with ribs (linear vertical alignment).